Clinical Guide

Recognizing and Understanding Skin Picking Disorder: A Guide for Professionals
Skin Picking Disorder (Excoriation Disorder), sometimes referred to as Dermatillomania, is a body-focused repetitive behavior (BFRB) characterized by recurrent picking of the skin that results in tissue damage, significant distress or impairment. Although it is a recognized mental health condition, it remains under-recognized across healthcare settings.
Professionals including therapists, counselors, social workers, dermatologists, physicians, nurses, and aestheticians may encounter individuals affected by skin picking without recognizing the condition. Developing an understanding of how skin picking presents, why it occurs, and how it affects individuals can support earlier identification and more effective intervention.
Why Providers Should Be Aware of Skin Picking Disorder
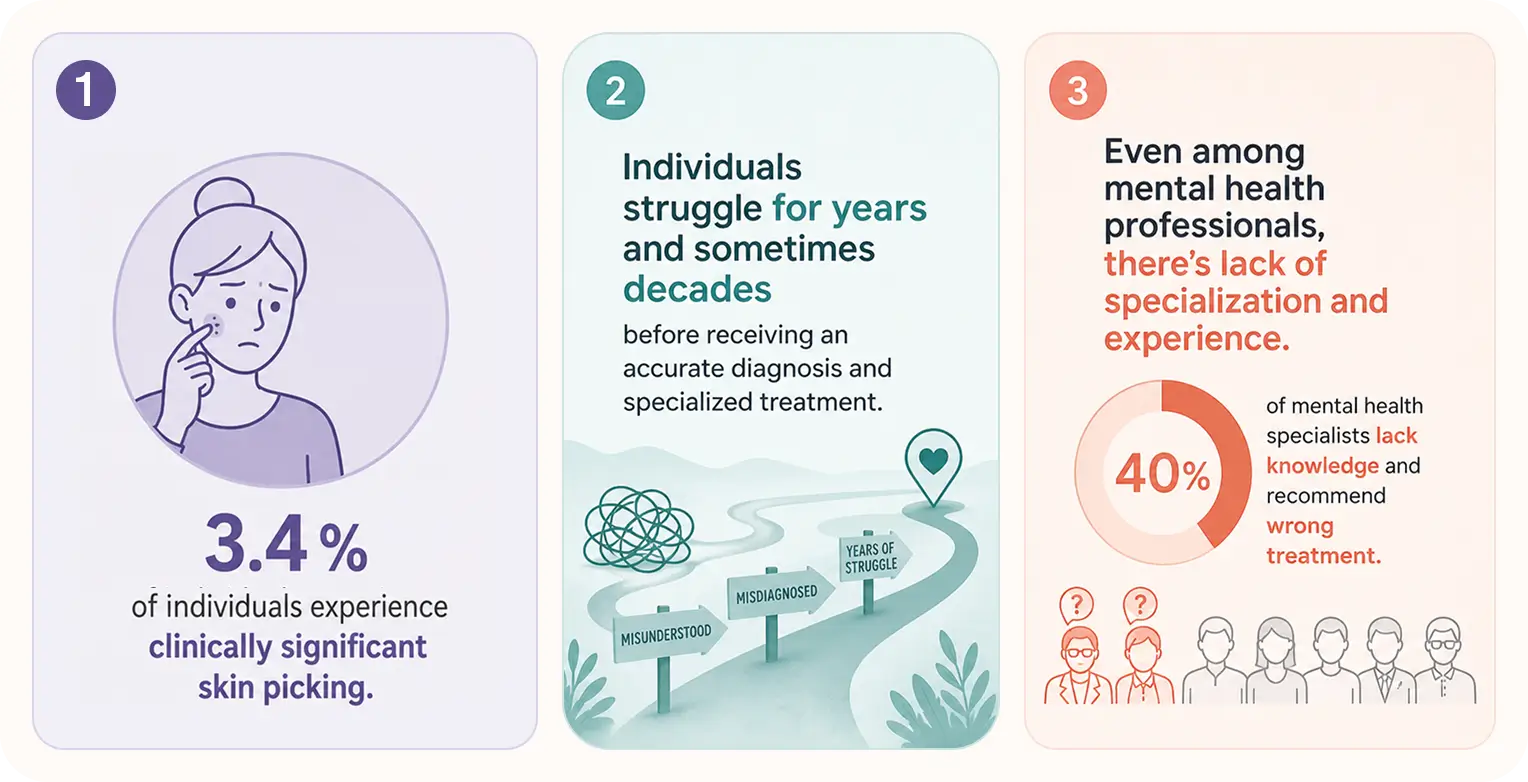
Skin Picking Disorder is more common than many professionals realize. A recent systematic review and meta-analysis estimated that approximately 3.4% of individuals experience clinically significant skin picking.
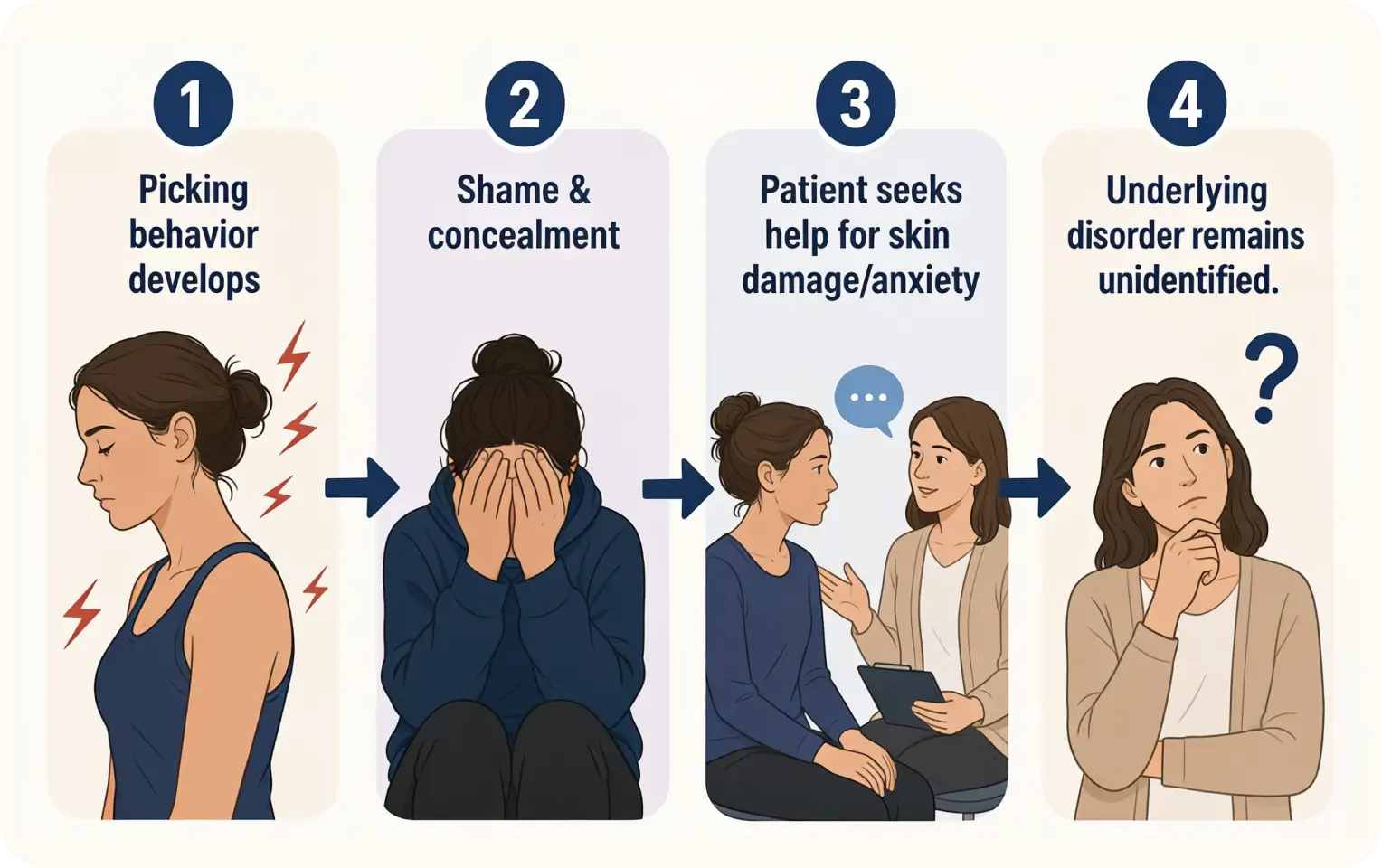
Despite its prevalence, many individuals struggle for years before receiving an accurate diagnosis or appropriate support. Some seek treatment for skin damage, infections, or scarring without disclosing the picking behavior itself. Others present with anxiety, depression, low self-esteem, or relationship difficulties while the underlying behavior remains unidentified.
Because shame and concealment are common, professionals may encounter Skin Picking Disorder more frequently than they realize.
What Is Skin Picking Disorder?
Most people pick at their skin occasionally - it is a common and normal self-grooming behavior. Skin Picking Disorder, however, differs in both frequency and impact.
Individuals with the disorder experience recurrent urges to pick and often report difficulty controlling the behavior despite repeated attempts to stop. Picking may focus on blemishes, scabs, rough patches, perceived imperfections, or healthy skin. Commonly affected areas include the face, scalp, hands, arms, shoulders, and legs, although any area of the body may be involved.
The consequences can range from mild irritation to significant tissue damage, infection, permanent scarring, emotional distress, and impairment in daily functioning.
Skin picking can develop at any age, but onset most commonly occurs during adolescence, often around puberty when acne and other skin irregularities become more prominent. Early identification is important, as untreated symptoms may contribute to physical complications, emotional distress, shame, and reduced quality of life.
The Role of Shame
One of the most significant yet frequently overlooked aspects of Skin Picking Disorder is shame.
Research suggests that many individuals experience feelings of shame, disgust, embarrassment, and self-criticism related to both the behavior and its visible consequences.
These experiences often extend beyond appearance concerns and can influence relationships, social activities, employment, and quality of life.
Many individuals go to considerable lengths to conceal affected areas of skin, avoid situations where their skin may be visible, or withdraw from social and intimate relationships. Feelings of shame and self-criticism may also contribute to a cycle in which distress increases the likelihood of further picking.
Understanding the role of shame can help professionals create a safer environment for disclosure, assessment, and treatment.
Current Understanding of Why People Pick
Current evidence suggests that Skin Picking Disorder is influenced by a combination of emotional, sensory, cognitive, behavioral, and environmental factors. For many individuals, skin picking may serve as a way of coping with difficult emotions, managing internal tension, or responding to sensory experiences.
It may temporarily reduce emotional distress, relieve tension, satisfy sensory needs, provide stimulation, or create a sense of satisfaction when perceived imperfections are removed.
Research also suggests that skin picking exists on a continuum between automatic and focused behavior. Automatic picking occurs with limited awareness, often while engaged in another activity, whereas focused picking occurs more intentionally in response to urges, emotions, sensory experiences, or perceived imperfections. Most individuals experience both forms.
Recognizing Skin Picking Disorder in Practice
Because shame and concealment are common, individuals may not voluntarily disclose their skin picking. Professionals may therefore need to ask directly, but sensitively, about picking behaviors when signs are present.
Potential indicators include:
- Recurrent wounds, scabs, scars, or skin infections
- Frequent touching, examining, squeezing, scratching, or manipulating of the skin
- Visible attempts to conceal affected areas
- Significant distress regarding appearance
- Feelings of shame, embarrassment, or secrecy
- Social, occupational, or relationship avoidance
- Reports of spending substantial amounts of time picking or thinking about picking
- Repeated unsuccessful attempts to stop picking
Individuals often seek help for the consequences of skin picking rather than the behavior itself.
Co-Occurring Conditions and Differential Considerations
Skin Picking Disorder often occurs alongside anxiety, depression, OCD, ADHD, other body-focused repetitive behaviors, and difficulties with emotion regulation.
It may also be confused with other conditions, including self-harm, dermatological disorders, Body-Dysmorphic Disorder, substance-related skin picking, or psychotic disorders involving delusional infestation. Understanding the function of the behavior, the associated distress, and its impact on daily functioning can help professionals develop an accurate conceptualization.
Evidence-Based Treatment Approaches
Several behavioral and psychological interventions have demonstrated effectiveness in the treatment of Skin Picking Disorder.
Evidence-based approaches include Habit Reversal Training (HRT), Cognitive Behavioral Therapy (CBT), Acceptance and Commitment Therapy (ACT), and Comprehensive Behavioral (ComB) interventions. These approaches focus on increasing awareness of picking patterns, identifying triggers, developing alternative responses to urges, and addressing the emotional, cognitive, sensory, and environmental factors that contribute to the behavior.
Self-monitoring is often a foundational component of treatment because it helps individuals identify triggers, urges, patterns, and high-risk situations. Effective treatment is typically tailored to the individual's unique experiences and maintaining factors.
Free tools for your patients
Learn about our personalized online therapy program, which empowers you to retrain your brain and find freedom from skin picking.
What Professionals Should Know
Perhaps one of the most important things professionals can understand is that Skin Picking Disorder is not a matter of willpower.
Many individuals have spent years blaming themselves, hiding their symptoms, and attempting unsuccessfully to stop. By the time they seek support, self-criticism and shame are often already deeply entrenched.
A curious, compassionate, and non-judgemental approach can make a meaningful difference. Understanding that skin picking often serves a function allows professionals to move beyond simplistic explanations and better support the individual sitting in front of them.
Final Thoughts
Skin Picking Disorder is a common yet frequently misunderstood condition. Greater awareness among healthcare and mental health professionals can contribute to earlier recognition, more compassionate care, and improved outcomes for those living with the condition.
Refer patient to SkinPick
Our treatment model is rooted in evidence-based approaches for BFRBs and delivered by therapists with extensive experience.
References
- Anderson, S., & Clarke, V. (2017). Disgust, shame and the psychosocial impact of skin picking: Evidence from an online support forum. Journal of Health Psychology, 24(13), 1773-1784. https://pubmed.ncbi.nlm.nih.gov/28810443/
- American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorders (5th ed., text rev.). https://doi.org/10.1176/appi.books.9780890425787
- Barber, K. E., & Fitzgerald, J. M. (2025). Emotion regulation deficits in skin picking (excoriation) disorder: A systematic review. Journal of Affective Disorders, 388, 119500. https://doi.org/10.1016/j.jad.2025.119500
- Mansueto, C. S., Goldfinger-Golomb, R., McCombs-Thomas, A. M., & Townsley-Stemberger, R. M. (1999). A comprehensive model for behavioral treatment of trichotillomania. Cognitive and Behavioral Practice, 6(1), 23-43. https://doi.org/10.1016/S1077-7229(99)80038-8
- Farhat, L. C., Reid, D., Bloch, M. H., & Olfson, M. (2023). Prevalence and gender distribution of excoriation (skin-picking) disorder: A systematic review and meta-analysis. https://pmc.ncbi.nlm.nih.gov/articles/PMC11137851/
- Gallinat, C., Schuck, K., Sadeghi, N., et al. (2024). Patterns of skin picking in skin-picking disorder: An ecological momentary assessment study. https://doi.org/10.2196/53831
- Moritz, S., Penney, D., Bruhns, A., Weidinger, S., & Schmotz, S. (2023). Habit reversal training and variants of decoupling for use in body-focused repetitive behaviors: A randomized controlled trial. Cognitive Therapy and Research, 47, 109-122. https://doi.org/10.1007/s10608-022-10334-9